In the world of SIU and No-Fault claim reviews, our team has learned one universal truth: sometimes the billing tells a more imaginative story than the operative report itself. And occasionally that story is so bold, so audacious, that it leaves us wondering whether we’re reviewing medical records or audition scripts for a daytime legal drama.
The Case of the Phantom MUA
One particularly memorable case involved an arthroscopic shoulder debridement procedure. Fairly standard on its face—until the billing arrived. Whether this counts as unbundling or phantom billing, we will leave to your SIU team to decide. What we can bring is the insight to review operative reports for language that easily triggers coding errors, whether intentional or accidental.
The provider didn’t stop at billing for the primary surgery. Instead, the provider appeared determined to maximize every possible line item of the surgery, including the injection procedure and fluoroscopic guidance codes which are inherently included in the main surgical procedure and even stated explicitly in the main procedure code descriptions. But our personal favorite code billed that day is CPT 23700-LT-59, Manipulation under anesthesia (MUA), left shoulder, distinct procedure.
Now, for those outside the coding trenches, manipulation under anesthesia (MUA) is typically reserved for cases where a patient develops significant postoperative stiffness or chronic restriction after conservative measures, like physical therapy and medication, have failed. In simpler terms, we are talking about a noninvasive procedure to treat chronic pain and break up scar tissue, performed when a joint becomes so stiff after surgery despite regular physical therapy and range-of-motion exercises. The key here is that it is performed after normal recovery methods fail to provide adequate relief.
For reference, most surgical procedures on a joint, whether open or arthroscopic, include the surgeon performing an intraoperative assessment of the joint by putting it through its normal range of motion to verify the procedure’s success. This is included in the global surgical package and does not represent a separate intervention.
Even simpler terms:
It’s a follow-up intervention, not a bonus feature during surgery.
The Plot Twist
The operative report itself was where things became especially entertaining.
First things first… The bill our team reviewed included MUA on the same date as the surgical procedure, although the operative report only mentioned applying a sling and briefly described passive stretching of the shoulder.
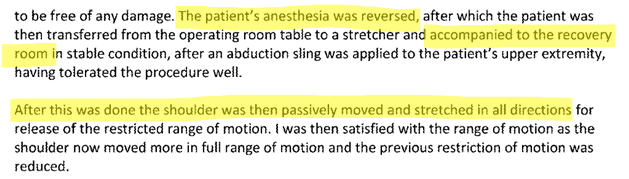
Now the juicy part. This moving and stretching of the shoulder was clearly described as being performed after anesthesia was ended (reversed) and the patient was transferred to the recovery room.
That’s right.
The billed “manipulation under anesthesia” reportedly occurred after anesthesia had already ended.
Which raises an obvious question:
Is it really “under anesthesia” if the anesthesia is over?
Don’t believe us? See for yourself!
This surgery was performed in December, so our team speculated that perhaps someone needed a little extra cash for Christmas. Unless holiday miracles were occurring in that operating suite, the answer is… probably not.
Surgical Reality vs. Billing Fiction
Routine intraoperative range-of-motion testing is a normal part of many orthopedic procedures. Surgeons commonly assess mobility before concluding surgery to confirm treatment success.
This is standard.
This is expected.
And most importantly:
This is included in the global surgical package.
Billing separately for basic post-procedural movement or passive stretching, particularly after anesthesia cessation, can trigger concerns ranging from unbundling to phantom billing.
We’ll let SIU decide which category fits best.
Why This Matters
Cases like this are precisely why detailed operative report review is essential.
Coding abuse doesn’t always appear as blatant fabrication. Sometimes it hides in:
- Mischaracterized procedural language
- Modifier misuse
- Distinct procedure overreach
- Global package violations
- “Creative interpretations” of documentation
And while we appreciate a good imagination, reimbursement systems generally prefer accuracy.
Final Thoughts from the Trenches
December surgery. Extra procedure. Questionable documentation.
Coincidence? Maybe.
Festive billing spirit? We’ll let you decide.
What we do know is this:
Our team routinely identifies questionable billing patterns that can expose providers engaging in:
- Unbundling
- Upcoding
- Phantom billing
- Modifier abuse
- Regulatory noncompliance
Because in SIU and No-Fault investigations, sometimes the biggest red flags aren’t hidden—they’re billed directly on the claim form.
Need an Extra Set of Eyes?
If your SIU team needs expert-level claim reviews with regulatory precision, coding scrutiny, and just enough sarcasm to stay sane, we’re here to help.
After all, you truly can’t make some of this up.